
An Epic Covid Fraud
How the largest hospital software vendor in the US biased the data

Why do Covid vaccines seem to be vastly more effective in the US than in the rest of the world? Because hospital software treats patients as “unvaccinated until proven otherwise.”
Epic
Epic is one of the largest electronic medical record (EMR) vendors in the world, based in Verona, WI. They employ about ten thousand people, and their software is used by a majority of healthcare providers in the US, including my former employer, Gundersen Health System in La Crosse, WI, where I worked as a nurse for nine years.
From Epic’s website:

Epic’s cornering of the EMR market means that much of our federal Covid data is filtered through Epic’s software.
Individual state vaccine registries are another piece of this puzzle: developed independently with no national standard, digital information sharing is tedious if not impossible.
How is this manifested at the patient level? During the Delta wave in 2021, staff at Gundersen saw a theme: if an out-of-state patient was hospitalized in Wisconsin, hospital software (Epic) would not check the vaccine registry of their state of residence, resulting in the patient being reported as “unvaccinated” to both the Wisconsin DHS and the CDC.
Epic’s Covid vaccine mandate
Is leadership at Epic objective about Covid? It appears not. For example, Epic has chosen an obtuse Covid vaccination policy for their staff:
We need our staff to be fully vaccinated to continue our important work. We will work with each employee to discuss how they can safely get vaccinated, but we recognize some employees may choose not to get vaccinated and hence will not be able to continue in their role.
In 2021, Epic, a tech company, imposed a vaccine mandate more strict than most hospitals, Pfizer, and the FDA. They implemented punitive testing requirements (three times a week) and fired or demoted unvaccinated staff. Epic still [3/28/2023] requires Covid vaccination for posted jobs:

While many other countries, corporations, and universities have backed off regarding vaccine requirements, Epic remains unjustifiably strict.
Epic and Vaccine Passports
Epic was eager to implement digital Covid vaccine passports that would require everyone to have Epic software on their smartphone:
First, the key to the vaccination codes is that they are not EHR-specific. They need to be readable by stadiums, airlines and other businesses, which require a safe method of confirming vaccination status.
Epic vaccine passports are QR codes displayed by Epic’s MyChart smart phone app and read by the SMART Health Card Verifier App at venues.
The justification for Covid vaccine passports is based on several assumptions:
Covid is a dire and imminent risk to everyone
Covid vaccines are safe
Covid vaccines are effective at preventing transmission
Covid vaccines are effective at preventing serious illness
Epic generated biased data supporting the need for vaccine passports while they positioned themselves to be the primary vendor for this new technology that would be mandatory for everyone, everywhere.
In a fragmented healthcare system, information is not shared easily or accurately.
Epic leadership has acknowledged the obstacles to accurately tracking the Covid vaccination status of hospitalized patients (my bold):
The pandemic shined a light on the lack of investment in healthcare data standards in the United States. The information immunization systems (IIS), of which there are more than 60, by and large do not talk to each other, and in many cases do not meet modern data needs.
While EHRs can transmit vaccine information between each other and to the state, we found many cases where the state IIS was unable to intake data on a real-time basis, or in some cases at all.
Solutions to this problem -a national registry with standardized data - are reportedly years away.
For me locally, the federal vaccines.gov website has 50 locations for receiving a Covid vaccine:

Walgreens, Target, Wal-Mart, clinics, hospitals, county buildings - they all have independent software systems. If you get a vaccination at Target, Walmart doesn’t know; no big deal. What is a big deal is when you are hospitalized with Covid, the hospital doesn’t always know you were vaccinated at Target, and then the CDC counts you as unvaccinated.
At Gundersen, patients vaccinated at the local VA would appear “unvaccinated” in Epic. Patients vaccinated at local nursing homes would appear “unvaccinated” in Epic.
One might wonder, when a person is hospitalized with Covid, isn’t it easy for hospital staff to just click if they are vaccinated or not?
No. Generally, when a patient arrives at a hospital unit, a nurse goes through an admission navigator with tabs of flowsheets. There is a tab for immunizations where you can review vaccinations on file, query the state immunization registry, and add missing immunizations. This process can be time consuming; for example, when you query the state registry, you might be waiting for minutes for a response. If the query times out, manually adding a historical vaccination is tedious. Updating immunizations is a low priority for direct patient care staff (especially given the nationwide staffing crisis).
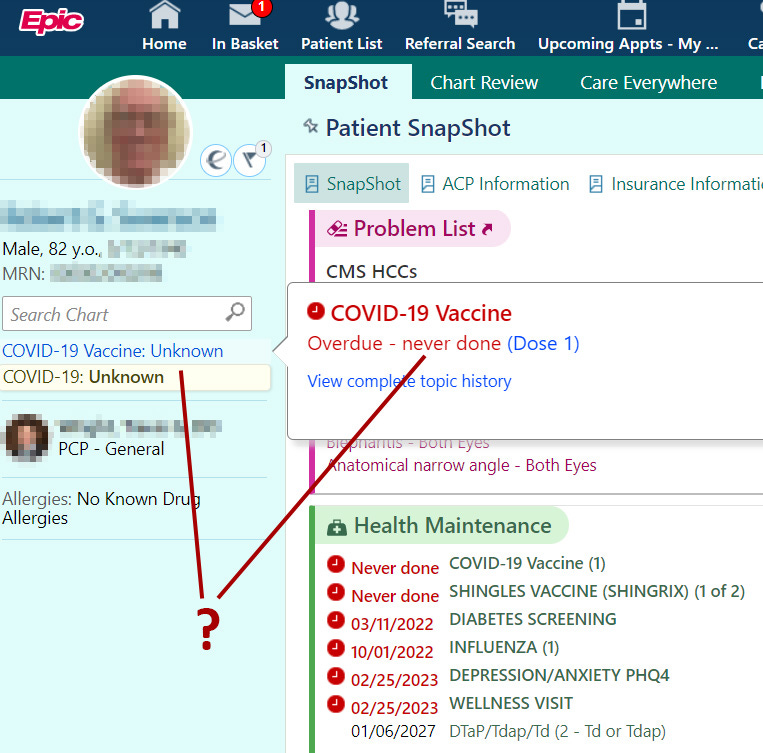
Unvaccinated until proven otherwise
During and after the mass Covid vaccination campaign, Epic software has only had two categories regarding Covid vaccination status: vaccinated and unvaccinated, with the default being unvaccinated. There was not an option for "unknown," which would have been more accurate; having an “unknown” vaccination status option was the approach in many other countries, like Switzerland.
CDC: https://covid.cdc.gov/covid-data-tracker/#covidnet-hospitalizations-vaccination
An unvaccinated person had Sars-Cov-2 RNA or antigen detected on a respiratory specimen and has not been verified to have received Covid-19 vaccine.
My bold - their default is “unvaccinated” instead of “unknown.”
The “unvaccinated until proven otherwise” software bias creates an overestimation of vaccine safety and efficacy. This bias then justifies authoritarian healthcare policy.

At Gundersen, Dr. Kowalski presented this information to staff at a Town Hall session just prior to the termination of unvaccinated staff.
Retrospective studies into vaccine injuries
Having "unvaccinated" be the software default doesn’t just contribute to an exaggeration of vaccine efficacy; it is also a smokescreen to assessing vaccine injury.
Vaccine injuries can be assessed on a large population of patients at once by a retrospective chart review: looking at an anonymized set of patient data for any new diagnoses following vaccination and comparing it to a control group. For example, if there is a statistically significant increase in myocarditis in the vaccinated group, that could be a signal of vaccine injury. A retrospective study can only be accurate if vaccination status is correct; if it's not, vaccine injuries will be undercounted. A biased retrospective analysis of vaccine safety has already been published by Epic:
Myocarditis Risk 17 Times Higher for Unvaccinated Patients Ages 12-30 Who Get COVID-19 Than COVID-Vaccinated Patients
We found the 30-day risk of myocarditis was less than the one-year historical incidence across all three vaccine manufacturers when considering all ages and sexes.
Astoundingly, Epic concluded that myocarditis was more common at baseline in 2019 than it was for vaccinated individuals in 2021:
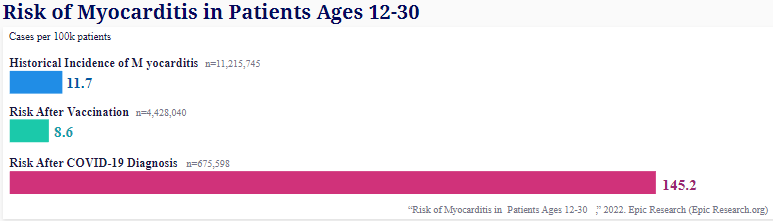
Epic would have us believe that vaccinated people have a rate of myocarditis below the pre-Covid baseline. This conclusion is wildly different from retrospective studies conducted elsewhere. It is unclear to me how Epic can be both self-aware of their data issues, as outlined in the article by Nick Frenser, while simultaneously putting out research that conflicts with both the rest of the world and common sense.
Nordic myocarditis study:

Note: Simpson’s paradox alert - this is total cases, not cases per 100k; the vaccinated pool is larger than the pool of the unvaccinated. It is presented to show a contrast to Epic’s similar study.
As study after study regarding myocarditis is published, Epic’s myocarditis data is the clear outlier.
Specific barriers to Epic data sharing at Gundersen Health System
When registering a new patient in Gundersen’s hospital software, it would require a Social Security number. When the SS# was unknown, registration staff would enter 111-11-1111. Data like this then becomes a barrier to sharing to/from outside systems (like the WI immunization registry) if the numbers don’t match; there are many safeguards put in place to prevent medical records from being merged incorrectly.
Both large hospitals in La Crosse - Mayo and Gundersen - use Epic. However, they have their own patient databases, and do not automatically crosstalk. There are ways to cross-compare patient charts, such as Care Everywhere, but that system has roadblocks and limitations.
Hospitals like Gundersen and companies like Epic display no insight into how their contributions to the Covid narrative and healthcare authoritarianism have worsened the frontline healthcare worker staffing crisis. I provided information for The Federalist about how Gundersen misled the local community about the impact to staffing caused by their vaccine mandate.
Epic themselves noted problematic trends in staffing, but not the connection to mandates:
‘The New Nurse’ Is the New Normal
Between March 2021 and March 2022, median nursing tenure fell by 19.5%.
Shifts covered by nurses new to the organization in the last 30 days increased in all regions.
The number of 12-hour shifts filled by nurses new to the organization within the last year also rose by 55.5%.
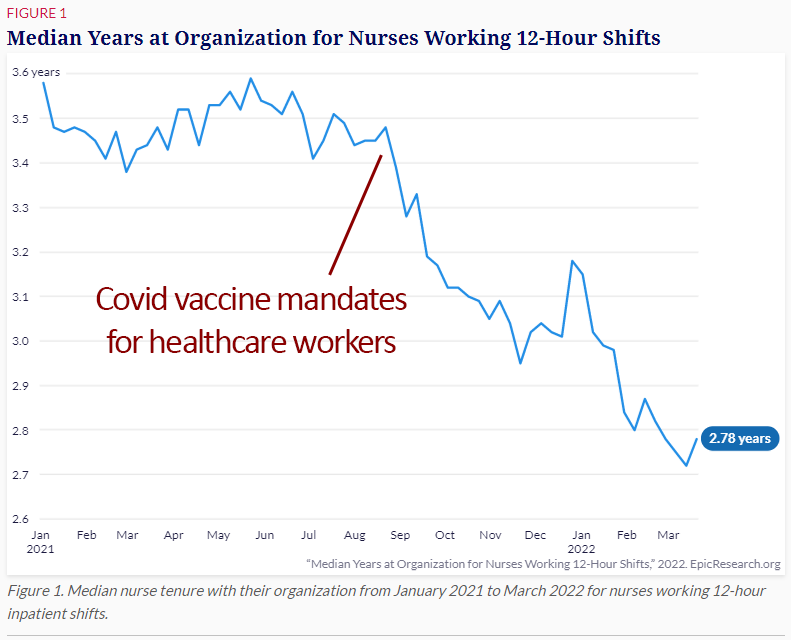
Red text added by me.
Being both sufficiently staffed and having staff with experience are by far the most important safety factors on a hospital floor. Covid vaccine mandates have caused a nationwide crisis. As of February 2023, the three nurses that were fired from my unit on just one shift have not returned to hospital nursing; two of us are no longer working as nurses at all.
Epic and VAERS
Epic has long been a pioneer of interoperability: helping fragmented software systems share nicely. However, this accurate information sharing has not been applied to either vaccination status or vaccine injury. Epic has made no efforts to facilitate or streamline the reporting of vaccine injuries to VAERS:

WITH vs FROM
Accurately capturing a person's vaccination status involves some barriers outside Epic’s control; it also involves distinguishing between patients hospitalized WITH Covid and those FROM Covid. Epic software had no way to distinguish patients with asymptomatic, incidental Covid. I worked with some of these patients myself on the psychiatric unit; they were counted as Covid hospitalizations, despite having no Covid symptoms. Epic does not have the functionality to distinguish. This lack of nuance comes directly from CDC guidance:
g) Asymptomatic individuals who test positive for COVID-19
For asymptomatic individuals who test positive for COVID-19, assign code U07.1,
COVID-19. Although the individual is asymptomatic, the individual has tested positive
and is considered to have the COVID-19 infection.
In a real-world example, psychiatric units like mine are notorious for being a financial burden on hospitals because a disproportionate number of psychiatric patients are uninsured or underinsured. However, with a Covid diagnosis, their hospitalization would be covered, even if asymptomatic. This “Covid” hospitalization then gets counted at the local, state, and national level, even if the person doesn’t have so much as a sniffle.
In May 2022, Epic made a hindsight attempt to distinguish “with” and “from” Covid:
A Bright Side: Hospitalizations for COVID-19 Might Be Overcounted, Especially Among Kids
These data come from Cosmos, a HIPAA-defined Limited Data Set of more than 138 million patients from 161 Epic organizations including 960 hospitals and more than 20,000 clinics, serving patients in all 50 states. This study was completed by two teams, each composed of a clinician and research scientists who worked independently.
Abstract: Most adult patients admitted with COVID-19 need treatment for COVID, but more pediatric patients are diagnosed with COVID-19 incidentally at admission.
Key Findings
Not all hospitalized patients who had COVID-19 were treated for COVID-19. They were likely hospitalized for an unrelated reason and happened to have COVID-19.
These incidental COVID-19 hospitalizations were highest during the omicron period when more than one-third of all COVID-19 hospitalizations did not include treatment for COVID-19.
Less than half of hospitalized pediatric patients who had COVID-19 were treated for COVID-19.
This Cosmos study is an acknowledgement of the problem by Epic themselves with no accompanying effort to fix it. There was much mainstream media fear mongering about the risk of Covid to children, particularly as vaccines were being approved and promoted. By Epic’s later estimate, a majority of pediatric hospital Covid cases were incidental.
How did their large overestimation influence vaccination recommendations and policy for children?
How did this affect reimbursement rates for those hospitalizations? Were hospitals paid for Covid admissions for all those incidental positive tests?
In 2020, insurers covered the costs of Covid hospitalizations. Taxpayers paid Medicare and Medicaid Covid hospitalizations. This changed after the vaccine rollout:
Earlier in the pandemic, relatively few COVID-19 patients would have been billed for their hospitalization because of the voluntary waivers extended by private insurers and employers. But as vaccines have become widely available to adults in the U.S. and health care utilization has rebounded more generally, health insurers may no longer face political or public relations pressure to continue waiving costs for COVID-19 treatment. As more waivers expire, more people hospitalized for COVID-19 – the vast majority of whom are unvaccinated – will likely receive significant medical bills for their treatment.
A false sense of vaccine safety and efficacy contributed to this widespread shift in policy, resulting in yet more persecution of the unvaccinated.
Per the CDC, we have had 7.5 million Covid hospitalizations. The average non-ICU Covid admission costs nearly $75,000. Epic estimates that “between 60% and 80% of all hospitalized COVID-19 patients were treated for COVID during their hospital admission,” meaning that 20-40% of patients were incorrectly counted (and billed) as a Covid hospitalization. Hospitals certainly had no financial incentive for nuance.
Wild napkin math:
75,000 x 7,500,000 = $562,500,000,000.00
If 20% were incidental Covid, that is $112,500,000,000.00
If 40% were incidental Covid, that is $225,000,000,000.00
What portion of those hospital bills were paid via taxpayers?
What portion of those hospital bills are being passed on to patients because the vaccine safety and efficacy was overestimated?
Does the CDC take incidental Covid into account with their calculations for hospitalization rates? Not according to Rochelle Walensky.

How can this problem be measured?
Can population-wide vaccination rate data be compared to the vaccination rate of various fragmented Epic datasets? For example, if La Crosse County is 65% vaccinated, what percent of La Crosse residents appear vaccinated in the Epic charts at Gundersen and Mayo?
Will Epic, Mayo, or Gundersen share, like Cleveland Clinic did, the prevalence of Covid illness amongst their own staff, by doses of vaccine given?
My anecdotal case
While in nursing school in 2011, I received vaccines for typhoid and yellow fever at UW-Madison Hospital, which uses Epic. It is logged in WIRS. My hometown hospital, Gundersen, also uses Epic - but does not have a record of my yellow fever vaccine. Asking MyChart to update from state registries does not pull in my typhoid or yellow fever vaccinations.
International comparison: Delta
In the last Town Hall prior to firing unvaccinated staff, Dr. Rathgaber, CEO of Gundersen, stated “Gundersen has the same experience with data being published all over the country… We aren’t any different than the rest of the world when it comes to the Delta variant of Covid-19.” Is this true? No.
In comparing the hospitalization rates of the vaccinated vs unvaccinated at the peak of Delta between the US, Finland, Slovenia, Ireland, and Switzerland, the US data is clearly the outlier. Their data is consistent to each other (2.5-2.9x difference), while the US data shows over a four-fold difference in vaccine efficacy (12.9x) at preventing hospitalization. Since these countries have universal healthcare, their data is more reliable than our fragmented system due to the issues listed above.
Does the bias created by Epic create this roughly four-fold overestimation of vaccine efficacy at preventing hospitalization in the US compared to the rest of the world?
If so, does this also confound the results of their safety studies by a similar proportion?
Other metrics of comparison include deaths by vaccination status and cases by vaccination status; for both these measures, the current CDC data is also significantly and persistently different than other countries.
International comparison: Omicron
Many states and countries took down their Covid data dashboards in mid-2022. This coincided with a noticeable depreciation in vaccine efficacy.
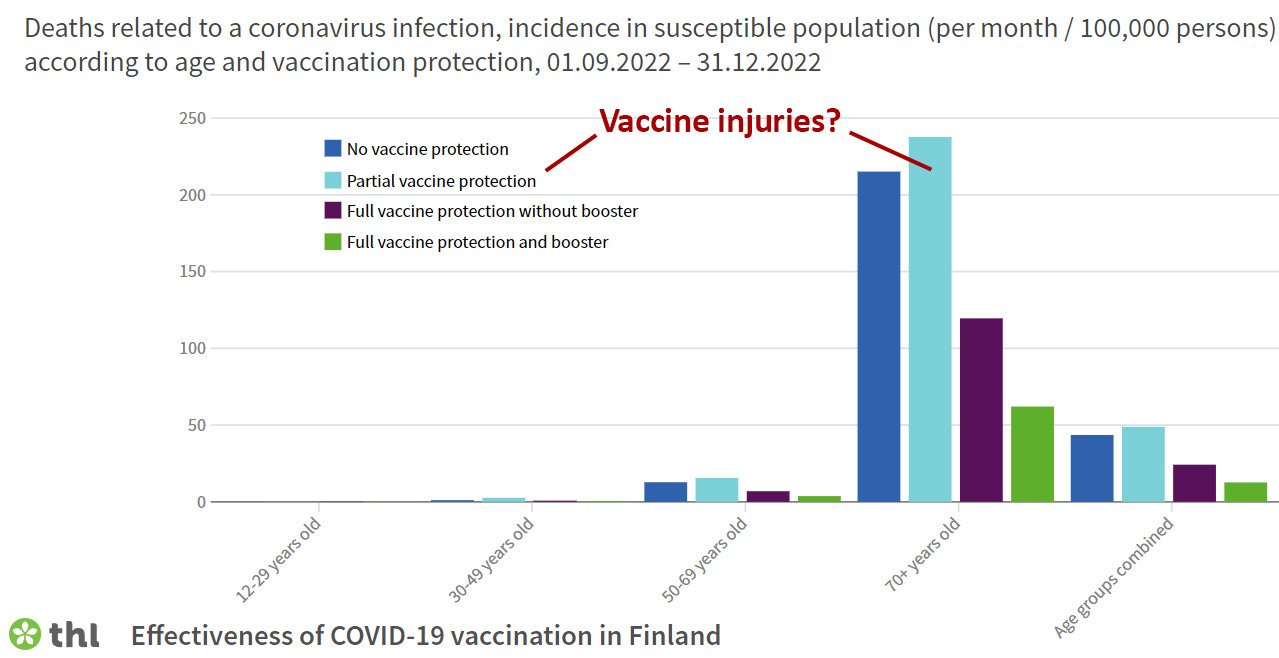
Just like Delta, the CDC’s estimate of vaccine efficacy during Omicron is wildly inconsistent when compared to those few other countries still sharing data. Look at cases and hospitalizations by vaccination status in the US compared to Switzerland and Finland; again, why are the vaccines seemingly so much more effective in the US? The few other countries still sharing their data show that the unvaccinated are getting Covid less often, being hospitalized less often, and dying less often than their vaccinated peers.
Finland’s data shows something else interesting: many people stopped after one dose, and they are generally not doing well. I would speculate that nobody gets dose one without intending to get dose two, and that these people stopped after one dose because they were injured; the increased mortality seen on the “partially vaccinated” group is because they have been damaged, and many had their lives shortened.
Finland data also shows that each Covid vaccine dose now increases the incidence of Covid infection:

This was also demonstrated by the recent Cleveland Clinic study:
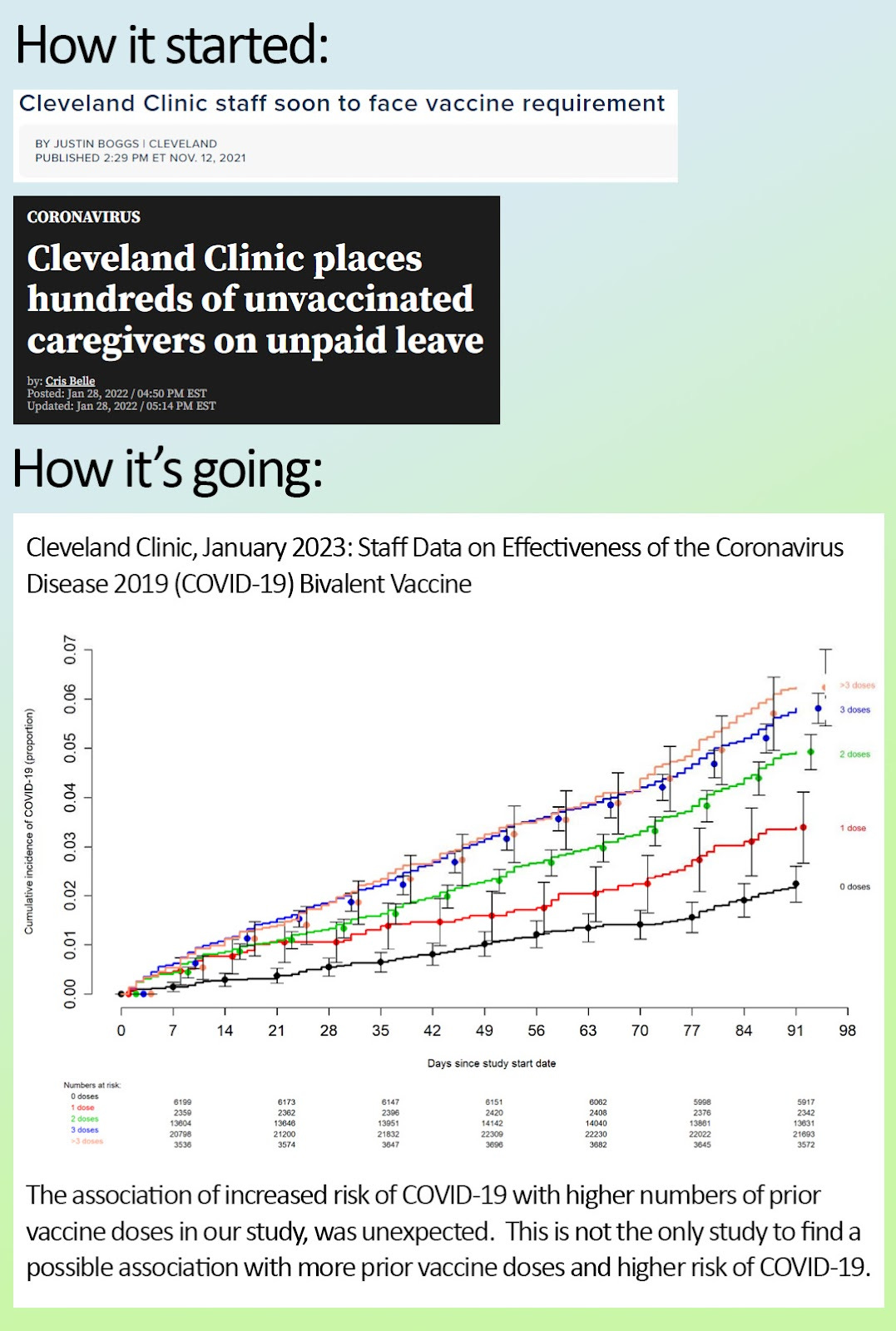
The Cleveland Clinic study is important because the 50k hospital staff were monitored for Covid much more closely than a random population of people. Studies that find Covid vaccines reduce transmission have many limitations not present in the Cleveland Clinic study.
This is in direct contrast to what Epic has claimed, using data from their own software:
VERONA, Wis. — Data collected by Epic Systems shows unvaccinated people are about 44 percent more likely than vaccinated people to get COVID-19 more than once, according to research released Tuesday.
Pick any country with universal healthcare and public data, and you will find a Covid story vastly different from ours. I have highlighted Finland and New Zealand because their data is publicly available, frequently updated, and easy to work with. Other countries have variable transparency.

Must adjust for Simpson’s fallacy since there are more vaccinated than unvaccinated.
We now see these other countries setting completely different Covid policy from the US. We are requiring vaccination for travel into the US; almost no other Western country is doing that. We are recommending Covid vaccines for six month old babies; in many European countries, they have moved to only recommending Covid shots for people age 50+ (ex. Denmark, UK), and even 65+ (Norway, Australia). Switzerland is now recommending against Covid vaccination for all ages.
Why is there a 64 ½ year difference between who the US believes is at risk from Covid, and who Norway believes is at risk from Covid? For those who say “follow the science,” what are our European counterparts seeing to have such wildly different Covid vaccine recommendations?
Other confounders
There’s much variability in how various countries present their data. Some lump one dose in with the unvaccinated, some have no category for “unknown,” generally you aren’t considered “vaccinated” until one to two weeks after your second dose (you are at an increased risk of infection immediately after your first dose). Got the jab, then immediately got Covid? Welcome to being counted as unvaccinated. Again, all this bias goes in one direction: overestimating vaccine safety and efficacy.
None of the nuances mentioned - like having separate categories for dose one and unknown, come close to explaining the difference in the US compared to the rest of the world. All measures of vaccine safety and efficacy show the US being the outlier.
It is also unclear how PCR test overcycling has also contributed to these data issues.
Others have dug into this as well, and it has been noted by Dr. Peter McCullough:

Results: We documented 25 instances when the CDC reported statistical or numerical errors. Twenty (80%) of these instances exaggerated the severity of the COVID-19 situation, 3 (12%) instances simultaneously exaggerated and downplayed the severity of the situation, one error was neutral, and one error exaggerated COVID-19 vaccine risks. The CDC was notified about the errors in 16 (64%) instances, and later corrected the errors, at least partially, in 13 (52%) instances.
Conclusions
Having accurate data regarding simple questions - was this hospitalized person vaccinated? - should not take a Manhattan Project level of effort. Yet here we are.
If I am wrong about Epic’s bias, WHY are Covid vaccines so much more safe and effective in the US than the rest of the world? Are there manufacturing issues? Are there unrecognized risk factors or protective factors at play? Why has excess mortality continued to rise unchecked since the mass rollout?
It strains the imagination to find a plausible explanation other than this: our Covid data is fatally flawed, those who make and wield that data are aware, and there is intention behind their failure to correct.
“Safe and effective.”
Anti-mandate rally outside Gundersen, September 4, 2021

David Anderson joining Mayo staff at their anti-mandate rally, January 3, 2022